What is bilingualism?
Bilingualism is defined as a speaker’s ability to use more than one language to communicate. For children growing up in bilingual environments, language acquisition is a dynamic journey influenced by the interaction of many differing linguistic inputs. Unlike monolingual children, who are exposed to a single linguistic system, bilinguals learn to differentiate between multiple languages and adapt their communication skills to diverse linguistic contexts. This process requires cognitive flexibility and a keen sensitivity to language cues from an early age.
Do Bilingual children acquire language in the same way that a monolingual child does?
Despite the complexity of bilingual language acquisition, research has shown that bilingual children typically achieve language milestones within a similar timeframe to their monolingual peers. From cooing and babbling in infancy to uttering their first words and eventually constructing complex sentences, bilinguals demonstrate a notable capacity for language learning and expression. Moreover, bilingual children often exhibit advanced metalinguistic awareness, allowing them to reflect on and manipulate language structures in both of their languages.
Code switching in Bilingualism
One of the defining features of bilingual language development is the ability to differentiate between and switch fluidly between languages. This is called code-switching. It is a natural and common phenomenon among bilinguals, serving various communicative functions and reflecting their linguistic versatility.
Challenges for Bilingual language development
Bilingual children may experience language mixing or blending, where elements of one language intrude into the other, particularly during the early stages of language acquisition. Additionally, bilingualism can sometimes be mistaken for language delay or disorder, highlighting the importance of accurate assessment and diagnosis by clinicians familiar with bilingual language development trajectories.
What can we do to help?
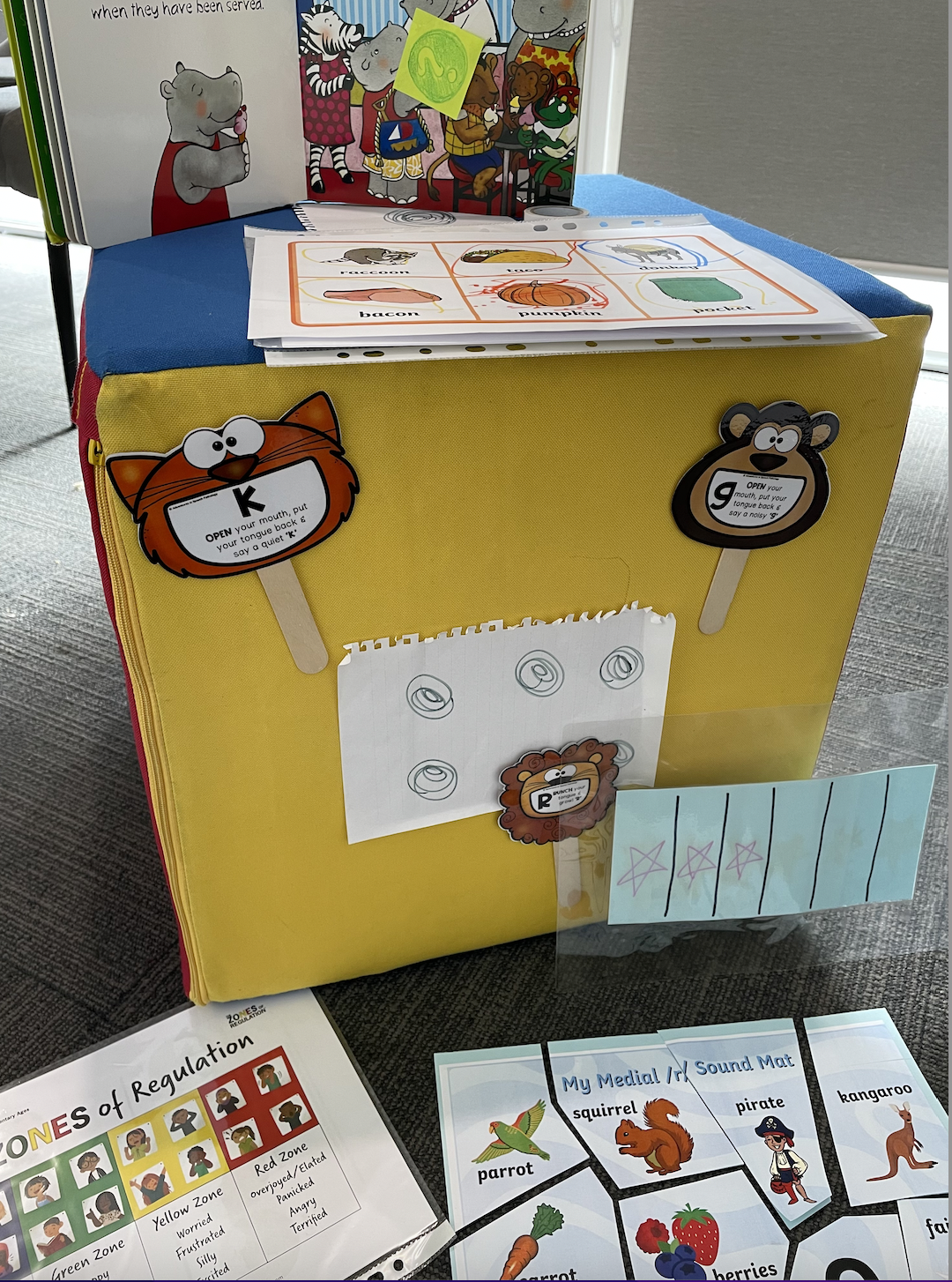
As caregivers, and speech pathologists, it is essential to provide bilingual children with a supportive and nurturing language-rich environment that promotes their language growth and development. Encouraging consistent exposure to both languages through meaningful interactions, storytelling, and culturally relevant activities can strengthen their language skills and promote balanced bilingualism. Moreover, valuing and affirming the child’s cultural and linguistic identity is of great importance in building positive self-esteem and a sense of belonging.
Written by Anna Roy, Allied Health Assistant (Speech Pathology), at De Silva Kids Clinic.




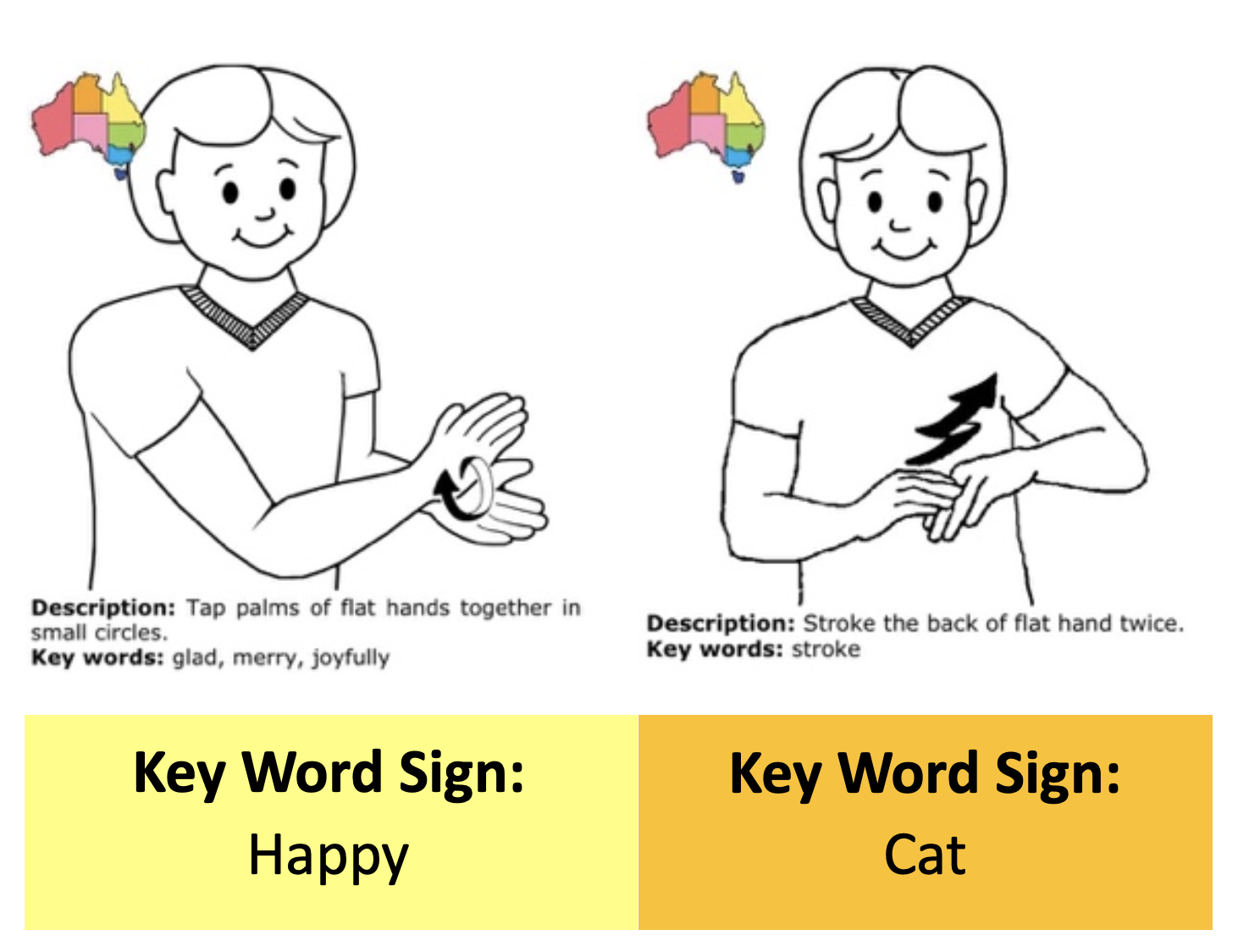
 You may ask yourself, “Well, what does it mean to create an environment that is rich in language?”. Let us unpack this with another question. What is language? Language is more than words. It is a socially shared system that goes beyond words. It is adaptive, generative, and multimodal. Think about it. If you were to search “new words in the dictionary 2023”, a list of words would appear. How else can we stay up to date with all these new words that kids are using these days? Otherwise, we would be termed pretty
You may ask yourself, “Well, what does it mean to create an environment that is rich in language?”. Let us unpack this with another question. What is language? Language is more than words. It is a socially shared system that goes beyond words. It is adaptive, generative, and multimodal. Think about it. If you were to search “new words in the dictionary 2023”, a list of words would appear. How else can we stay up to date with all these new words that kids are using these days? Otherwise, we would be termed pretty